The Best Hip Impingement Guide On The Internet
Jul 19, 2023
Hip pain, pinching, and/or Femoral Acetabular Impingement (FAI) of the hip is no fun, but if you or a client of yours is experiencing this issue, fear not - there is hope.
In this article, I will discuss:
- The three most common types of hip impingement
- Common & expected test results for each type
- Strategies to improve movement quality
Before I begin addressing hip impingement, I want to make it clear that if this is a specific diagnosable condition, please be sure to work alongside a qualified physical therapist. Trainers do not have the ability to diagnose and treat pain, but we can program responsible exercises to improve movement. This article is for educational purposes only and is not meant to serve as a means of self-diagnosis.
The information in this post was significantly influenced by my favorite Postural Restoration Institute course: Impingement & Instability.
Determining Asymmetry
If you've ever seen my content before, it's likely you are familiar with my belief that no two sides of the body are equal. Every single human is asymmetrical to some extent, which will influence how a similar issue can arise depending on which side the problem is on.
The types of hip pinching and impingement I am going to describe below tend to occur on one side more than the other, so it's important to know which type of impingement you have so you can choose the best solutions.
Every human has a bias towards leaning to one side, the left or the right. This means that we are more "lateralized" to that side and therefore more weight-bearing on that side.
We will be using a few different tests to understand which side that is.
The side we are leaning on will be generally more internally rotated, and the side we are shifted away from will be relatively more externally rotated.
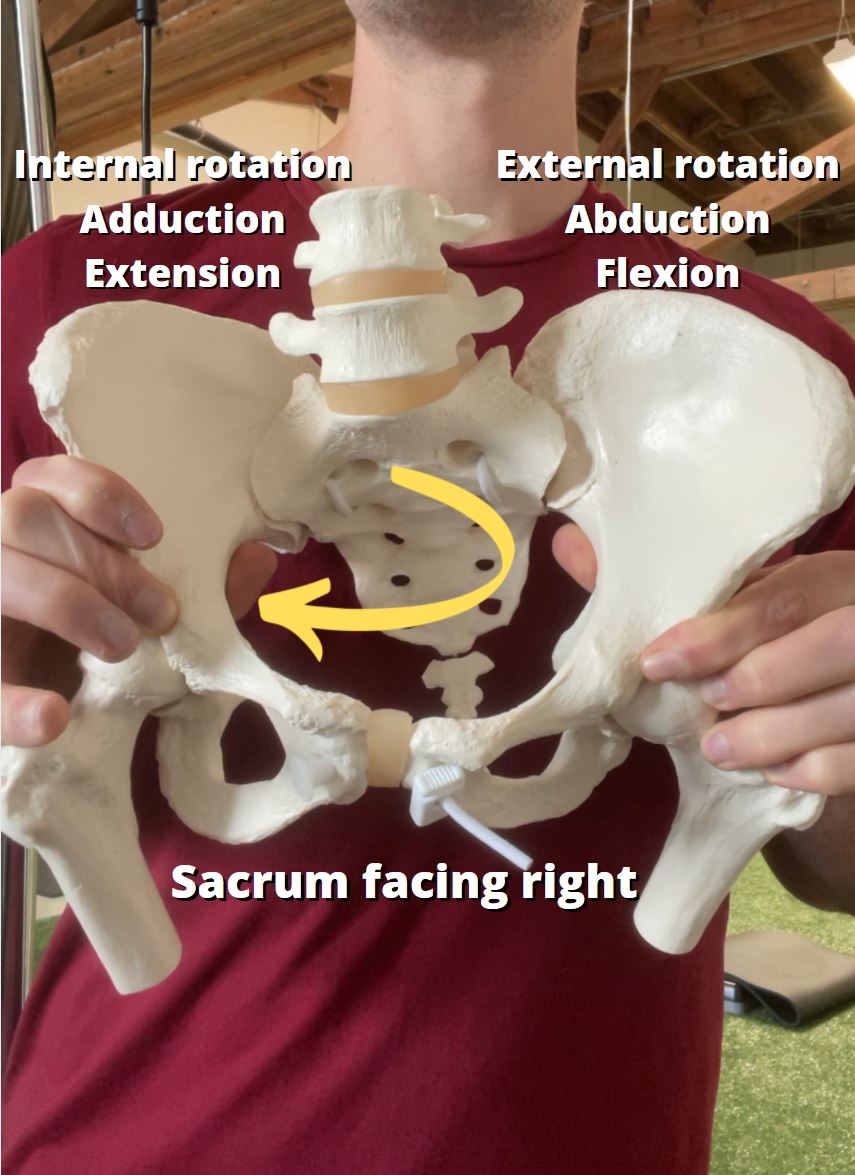
The side that is more internally rotated will be associated with certain types of issues and impingements, and the more externally rotated side will have its own common biomechanical biases as well.
Use these tests to determine that. Most people will have a bias towards more right hip internal rotation and left hip external rotation because of our natural asymmetrical pattern which you can read more about here, the Left AIC.
Straight Leg Raise: This is a test of hip internal rotation.
Hip Flexion: This is a test of hip external rotation.
Femoral Internal & External Rotation:
Shoulder Abduction: This is a test to determine which side you will be turned towards. The side you are lateralized to will have better abduction.
Given there are five total tests, you will have at least 3/5 indicating you are lateralized towards that side. Go with that one.
For example, if I was more lateralized to the right, I would have:
- Straight Leg Raise: L < R
- Hip Flexion: L > R
- Femoral Internal Rotation: L < R
- Femoral External Rotation: L > R
- Shoulder Abduction: L < R
The Different Types of Hip Impingement
There are obviously so many different iterations of impingement, but for the purposes of simplicity, we can break them down into three main types:
Type #1: Anterosuperior Acetabular Impingement
In this type of hip impingement, what we often see is a pelvic innominate bone that is very anteriorly oriented ("anterior pelvic tilt") and externally rotated on the side of the impingement.
In this case we often see this coupled with compression of the posterior (back) side of the pelvis. The reason for this is that because the pelvis is so far forward on that side, the back of the pelvis starts to tighten up to help "pull" the pelvis back, but this actually results in the femur being pushed forward within the acetabulum (hip socket).

Therefore, this impingement will be most apparent when the individual tries to internally rotate the femur via pushing it back within the acetabulum.
The femur will get stuck on the superior (upper) part of the hip socket.
Because the left side of the pelvis is usually more forward than the right (see my content on the Left AIC for more on why), this type of impingement usually happens on the left side.
Common Test Results
In this case, we would often see the following issues on the limited side:
- Straight Leg Raise: 45 degrees or less
- Hip Flexion: Less than 110 degrees (usually around 90)
- Femoral Internal Rotation: Less than 20 degrees
- Femoral External Rotation: More than 25 degrees
Type #2: Anteromedial Femoral Acetabular Impingement
In this case, the femur is going to be feel "pinchy" (impinged) when it tries to internally rotate, but for a different reason than above.
The femur is going to be restricted going into internal rotation because it is essentially already pushed back in the acetabulum.

The femur is likely already starting in a position of adduction and internal rotation, which biases it towards a position where it is posteriorly rotated.
More internal rotation creates the impingement sensation because "you can't get somewhere you're trying to go if you're already there".
Because the right side tends to be in more internal rotation, this occurs more often on the right side.
In this case, we would expect to see on the limited side:
- Straight Leg Raise: Around 50-70 degrees
- Hip Flexion: Less than 100 degrees (usually around 90)
- Femoral Internal Rotation: More than 20 degrees
- Femoral External Rotation: Less than 25-30 degrees
Additional Considerations:
In many cases, people have these asymmetries, but also have an overall pelvic orientation which is stuck in an anterior pelvic tilt. This means that both sides of the pelvis are forward, but one side of the pelvis is still more forward than the other.
So you will have the lateralization towards one side still, but both sides will present with limited measurements. In these cases, you'll usually see on both sides:
- Hip Flexion: Less than 100 degrees (usually around 90)
- Femoral Internal Rotation: Less than 25 degrees
- Femoral External Rotation: Less than 30 degrees
- Shoulder Abduction: Less than 40 degrees
If this is the case for you, I would recommend doing something to first improve the position of the pelvis on both sides before addressing asymmetry. Do whichever of these two feels easiest:
Exercises for Hip Impingement
Here are some exercises that can help improve movement quality so that dynamic activities such as gait and weightroom training can become easier. I will address each of the following types as presented in the order above.
If you're looking for more strategies to improve movement to help your clients feel great, check out my free webinar: 5 Strategies To Help Your Clients Feel 85% Better Immediately
Type #1: Anterosuperior Acetabular Impingement
The goal with this is to get the femur to be able to slide back within the acetabulum and get the pelvis to access more genuine hip internal rotation. The following exercises are presented in order of difficulty:
Type #2: Anteromedial Femoral Acetabular Impingement
For this type of impingement, we want to push the femur into more external rotation and also allow the pelvis to create more external rotation as well via muscles such as the lower right glute max.
In this context, the opposite side of the hip usually has limited internal rotation, so we can improve that as well to restore more overall neutrality to the pelvis:
Summary
These are the most common types of hip impingement we see as they relate to natural human asymmetrical patterns. Usually the problem is that the femur is being pushed into a certain position because the position of the pelvis as a whole (both sides included) are creating an orientation of the hips that shift the femur in that specific position.
The femur will then struggle to move into a position outside of that orientation (or be limited in moving further into it), which results in that femur being jammed on a specific part of the acetabulum.
If you are experiencing these issues, first see a qualified Physical Therapist who appreciates how asymmetry can affect hip impingement. Please do not try to self-diagnose.
Don’t miss out on free education
Join our email list to receive exclusive content on how to feel & move better.
